The Blog
Last blog published in October 2017.
For more recent articles, visit The Tisserand Institute.

In defense of science, and of safety precautions
In a recent blog post Jade Shutes challenges the safety guidelines for using essential oils in the bath published on TisserandInstitute.org. She also feels that there is an increasing (and in her opinion unfortunate) trend to cite research. Jade proposes that this is...
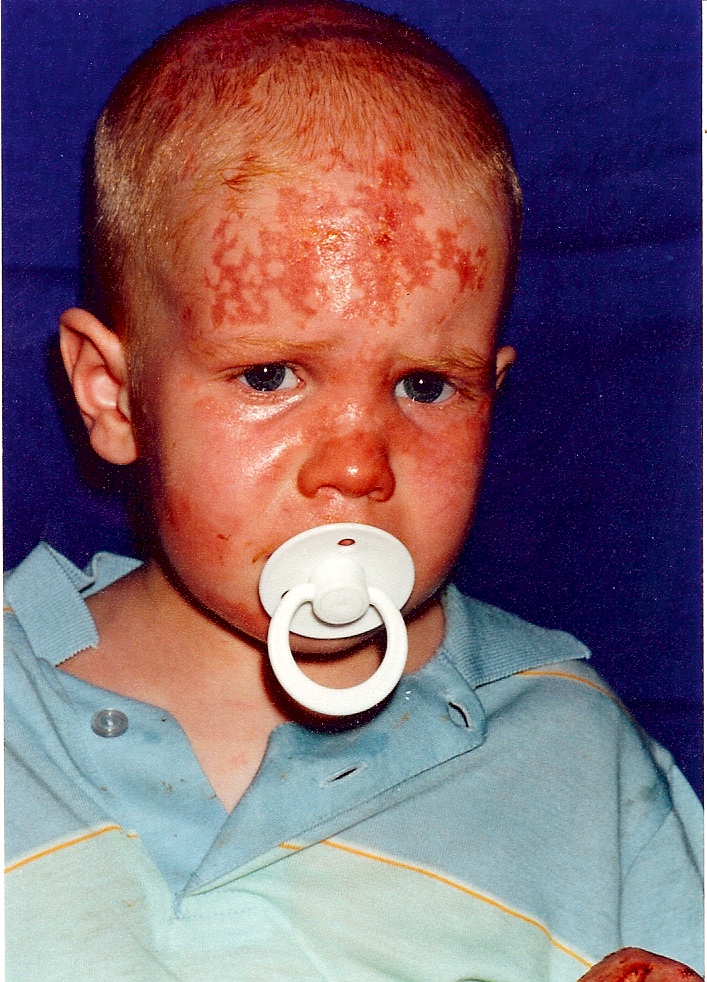
Lavender Helps Burned Boy – a heart-rending story with a happy ending!
In the winter of 1994, I was contacted by a Mandy Kelly, whose little boy Ciaran had been badly burned in an accident involving a wood-burning stove. Apart from wanting to do anything to help him heal, she was also an aromatherapy enthusiast. She called me and I...

Essential Oils and Seasonal Affective Disorder
by Robert Tisserand Feeling unusually sad is not uncommon in the winter months. Classic (winter based) seasonal affective disorder (SAD) is a mood disorder, affecting people with otherwise normal mental health. Symptoms include difficulty waking up in the morning,...

Robert Tisserand interviewed on ingestion, dilution and other safety issues
In December 2014 I was interviewed by Labron Allen, a functional medicine nutritionist based in Texas, for his Health Alert radio show. This is a full transcript of the podcast, which you can find here or here. Many thanks to Anne Bankowski for the transcription. I’m...
Frankincense essential oil and cancer: Why EOs and chemotherapy don’t always mix
Hi, My friend just started taking chemo for colon liver cancer and she was taking therapeutic Sacra Frankincense from Young Living before she started. I read somewhere that you should not take the essential oil with 5FU if you are taking it for skin cancer because it...
Lavender mascara?
Adding lavender oil to your mascara has become a thing, on the basis that it will make your eyelashes longer and thicker, and also that it will deter eyelash mites. About half of us have tiny eyelash mites, but they don't affect at least 95% of those who have them....
Bergamot Oil – Toxic To Children?
I was recently contacted by an essential oil business (Plant Therapy) which had several customers ask about the safety of bergamot oil, as they had heard it could be lethal and cause convulsions in children. The sources of this warning appear to be MedicineNet.com and...
China Report 2014
On Thursday July 24th, I left home for my second visit to the People's Republic of China! (see report and video of my first visit here, and pics here) This time I was invited by a Beijing-based aromatherapy school, Floralwish. The most obvious difference from my 2011...
Essential oils and gut flora
In a blog post dated July 13th 2014, Madhupa Maypop quoted Paul Bergner, saying: “The scent of an essential oil can kill gut flora just like antibiotics do, according to Paul Bergner, director of the clinical studies program at the Rocky Mountain Center for Botanical...